About Us and How To Contact Us
The overarching purpose of the Lewisham Safeguarding Adults Board (LSAB) is to help and safeguard adults with care and support needs by:
- Assuring itself that local safeguarding arrangements are in place as defined by the Care Act 2014 and statutory guidance;
- Assuring itself that safeguarding practice is person-centred and outcome-focused;
- Working collaboratively to prevent abuse and neglect where possible;
- Ensuring agencies and individuals give timely and proportionate responses when abuse or neglect have occurred; and
- Assuring itself that safeguarding practice is continuously improving and enhancing the quality of life of adults in its area.
The Board meets four times a year and has an Independent Chair.
In Lewisham the Board believes that "Safeguarding is Everyone's Business". Its pledge to the people in Lewisham is that by working together and in partnership the risk of abuse or harm can be reduced by raising awareness of safeguarding of adults. As intelligence is gathered from across the partnership activity trends can be analysed and areas of concern identified so that preventative measures can be applied to keep people safe.
There are two ways that you can get in contact with us, by email or letter.
Email Us
Postal Address: Lewisham Safeguarding Adults Board, C/o London Borough of Lewisham, 3rd Floor, Laurence House, Catford, London, SE6 4RU.
**Do not contact the Independent Safeguarding Adults Board to report Safeguarding Concerns. You need to contact Adult Gateway at Lewisham Council. Please see "How to Report a Adult Safeguarding Concern" page. Please also consider the transmission of personal information when making a referral to the Council. **
How to Report a Adult Safeguarding Concern
Please visit our How to report your Concerns page.
You can also follow us on Twitter @lewisham_sab
Safeguarding Adults Reviews & How to Make a Referral
Lewisham Safeguarding Adults Board (LSAB) will arrange a Safeguarding Adults Review (SAR) when an adult in Lewisham dies as a result of abuse or neglect, whether known or suspected, and there is concern that partner agencies could have worked more effectively to protect the adult.
We will also arrange a SAR if an adult in Lewisham has not died, but the LSAB knows or suspects that the adult has experienced serious abuse or neglect.
We are also free to arrange for a SAR in any other situations involving an adult in Lewisham with needs for care and support.
The Department of Health's Safeguarding Care and Support Statutory Guidance guides the reviews we carry out.
Should the LSAB carry out a review we have a LSAB SAR Policy & Procedures October 2023 that we work to, which explains in detail what you can expect us to undertake for the Lewisham Community.
The National SAB Guidance on the Interface between SARs and Coronial Processes - September 2024 provides guidance on how we work with HM Coroner.
Read our published Safeguarding Adult Reviews.
Make a referral to the Board for a Safeguarding Adults Review
If you would like to refer a case to us for the boards consideration for a Safeguarding Adults Review to be commissioned please use our dedicated notification form.
LSAB Structure and Members
Organisations represented on the LSAB
- Age UK Lewisham and Southwark
- Change Grow Live (CGL)
- Department for Work and Pensions – South London District
- Healthwatch Lewisham
- Lewisham & Greenwich NHS Trust
- Lewisham Adult Social Care
- Lewisham Speaking Up
- Lewisham Refugee and Migrant Network (LRMN)
- Lewisham Safeguarding Children Partnership (LSCP)
- Lewisham Housing Directorate
- Lewisham Adult Integrated Commissioning
- Lewisham Safer Communities
- London Ambulance Service NHS Trust
- London Fire Brigade
- Metropolitan Police Service, Lewisham (South East BCU)
- National Probation Service, Lewisham and Bromley
- NHS South East London Integrated Care Service and Board
- South East London MIND
- South London & Maudsley NHS Foundation Trust
There will also be representatives from partner agencies on Sub-Groups.
Governance
The LSAB is responsible for ensuring organisations are meeting their safeguarding obligations effectively and will hold them to account if they are not.
As individuals, Board members are accountable to their own agencies but the Board as a whole will be accountable to the Department of Health and Social Care, and provides reports locally to the Health and Wellbeing Board and the Healthier Communities Select Committee.
Its work may be scrutinised periodically by the Overview and Scrutiny Committee and is liable to be inspected at any time by the Care Quality Commission (CQC).
The Board, through the independent chair, is accountable to the Chief Executive of the Local Authority, the Chief Executive of the NHS Integrated Care Board (ICB) and the Borough Commander of Police.
These Executive Group of agencies may periodically meet to discuss the strategic direction of the Board, and additionally invite the London Fire Brigade Borough Commander, Chief Executive of Lewisham & Greenwich NHS Trust, and Chief Executive of the South London & Maudsley NHS Foundation Trust to join this group.
Lewisham Safeguarding Adults Board Structure
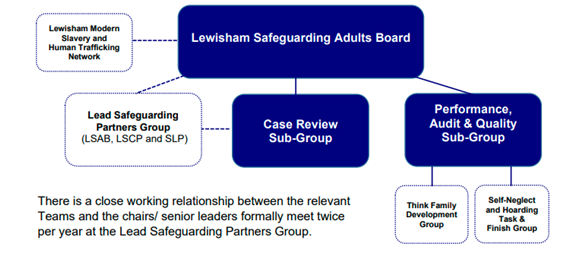
The LSAB Compact and Strategic Business Plan 2025-2026 describes how these organisations and their representatives on the Lewisham Safeguarding Adults Board (LSAB) will work together in partnership to safeguard the residents of Lewisham in 2025-26.